The Hidden Architecture of Your Neck: 5 Surprising Truths from Clinical Biomechanics
The High-Stakes Balancing Act
Think of your head not merely as a part of your anatomy, but as a high-altitude "sensory platform." It houses the critical hardware for vision, hearing, smell, and taste—tools that must constantly scan the environment with precision. To function, these organs require the head to be delivered toward objects of interest in three-dimensional space.
The cervical spine is the specialized engineering device that subserves these facilities. Its central challenge is a fascinating paradox: it must be flexible enough to allow for rapid sensory scanning, yet stable enough to protect the vital neural pathways and the heavy "platform" it supports. To truly understand why the neck hurts or how it moves, we have to look past the surface and into the unique, counter-intuitive biomechanics revealed by modern clinical research.
1. The Atlas Paradox: The Bone That Moves Its Own Way
At the very top of your spine sits the first cervical vertebra (C1), known as the Atlas or "The Cradle." Its primary job is to nurse the base of your skull through every movement. However, the Atlas behaves unlike any other bone in your spine because it acts as a "passive washer."
Remarkably, the Atlas has almost no muscles that act directly upon it to create independent movement. Instead, it is governed by the muscles acting on the head above it. This leads to "paradoxical motion": while you might assume all vertebrae move in the same direction during a tilt, the Atlas can actually extend (tilt backward) even as the rest of your neck flexes (tilts forward). As the Bogduk and Mercer research explains:
"Sandwiched between the head and axis, and balanced precariously on the summits of the lateral atlanto-axial facets," the atlas is subject to pure compression.
If the weight of the head falls behind the balance point—as it often does when we "tuck" our chins—the Atlas tilts backward, regardless of the neck's overall direction. For a manual therapist, this means the C1 level may feel "extended" or "stuck" even when a patient is in a flexed posture, a mechanical quirk of loading rather than a structural injury.
2. Why Your X-Rays Might Be Lying to You
Standard medical imaging, like X-rays, provides a helpful but flat and incomplete picture. When viewing a side-view radiograph of the joints between the Atlas and the Axis (C2), the surfaces often appear perfectly flat, suggesting the bones simply slide across one another like two plates.
In reality, the anatomy is far more sophisticated. While the bone beneath may look flat, the articular cartilages covering them are "biconvex"—curved outward on both the top and bottom, much like the shape of a lentil or two shallow hills meeting. Because of this biconvexity, the joints don't just slide; the Atlas actually "nestles" or descends into the Axis during rotation. As you turn your head, the Atlas slips down the slopes of these cartilaginous curves, rising back to the summit only when you return to center. This "nestling" is a vital mechanical detail that standard film cannot capture, yet it is essential for the smooth, "greased" rotation of our head.
3. The "Broken" Disc: A Design Feature, Not a Bug
In the lumbar spine (lower back), a "cleft" or tear in a disc is often a red flag for injury. However, the cervical spine follows an entirely different blueprint. Cervical discs are not built with the full concentric rings of fibers (the annulus fibrosus) found in the lower back. Instead, they are part of a specialized "saddle joint" system.
Fissures in cervical discs are not necessarily signs of decay; they are developmental milestones. These clefts actually commence as early as age nine and are typically complete by the third decade of life. Rather than pathological decay, this is "programmed attrition." Because the back of the disc is essentially split, the vertebra is free to swing and pivot around its front end, facilitating the wide range of rotation we require.
This movement is kept safe by the uncinate processes—bony ridges on the sides of the vertebrae that act like the "side rails" of a cradle. These rails allow the disc to have its functional cleft while ensuring the "saddle" stays on track, preventing the vertebrae from sliding off those biconvex slopes.
4. The Myth of the "Normal" Range of Motion
We often speak of a "normal" range of motion (ROM) as a fixed goal for health. However, clinical biomechanics reveals that ROM is surprisingly inconsistent. Research shows that an individual’s range varies significantly based on the direction of movement; the total distance measured when moving from a forward-tilt to a back-tilt can differ by 10 to 30 degrees compared to the reverse.
Furthermore, these measurements are not stable over time. Even in the same healthy individual, the range of motion can fluctuate by more than 5 degrees when measured just 10 weeks apart. "Normal" behavior is not a single value to be "hit," but a range of variation that changes with a person’s daily strategy and timing.
5. Quality Over Quantity: The Invisible Map of Pain
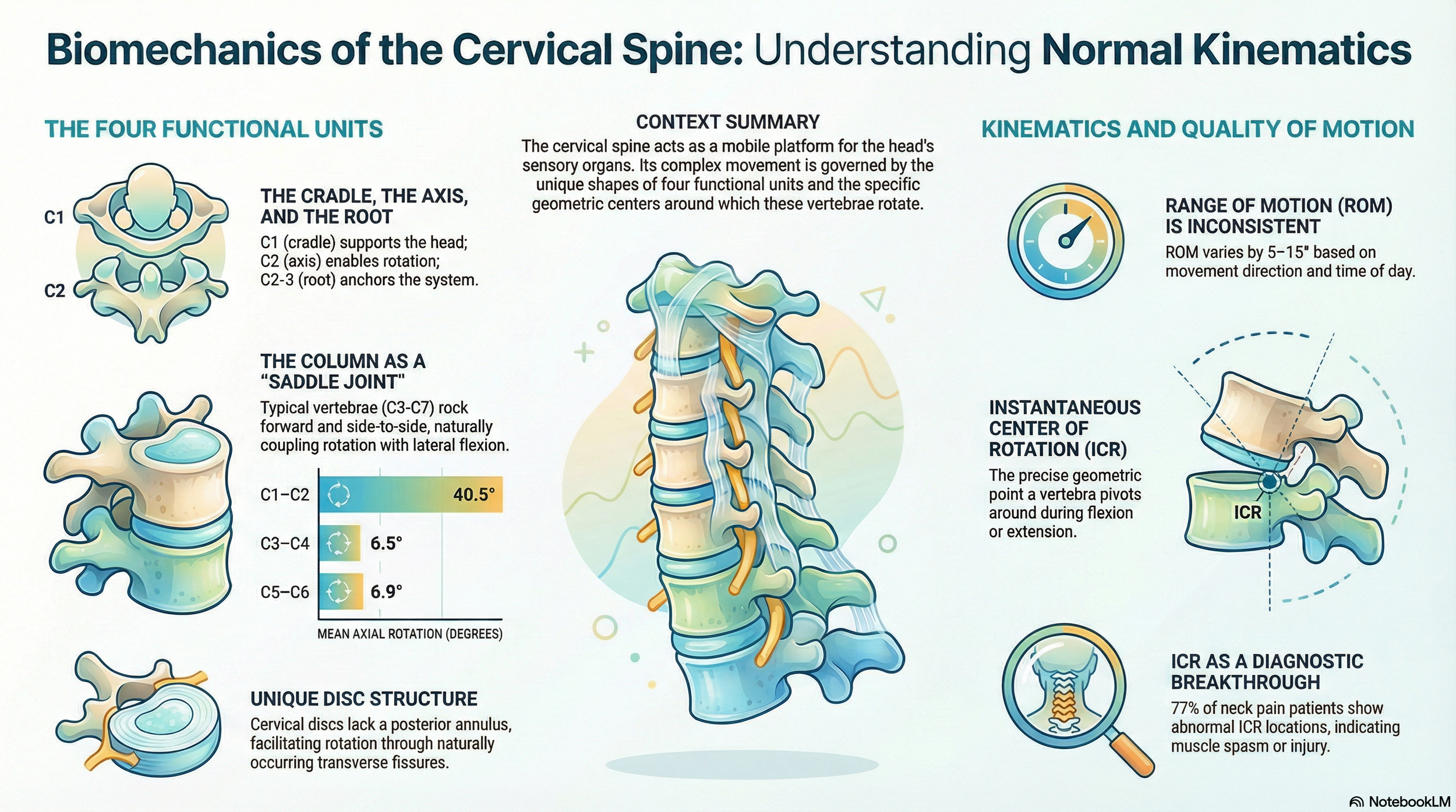
If total range of motion is an inconsistent metric, how do we identify a problem? The answer lies in the "quality" of motion, measured by the Instantaneous Centre of Rotation (ICR). Think of the ICR as the "eye of the storm." While the head moves in a wide arc, the ICR is the stable pivot point around which the vertebra rotates.
In healthy individuals, the "eye" remains remarkably stable. However, the discovery is "highly significant": 77% of patients with post-traumatic neck pain have abnormally located ICRs, even when their total range of motion appears perfectly normal. The movement may look full, but it has become "turbulent" because the pivot point has shifted.
An abnormal ICR is a "strong sign of increased posterior muscle tension" that acts like "invisible planets" affecting motion.
Just as an invisible planet is detected by the gravitational pull it exerts on nearby stars, we can detect the presence of hidden muscle spasms by how they yank the ICR out of its stable orbit. This shift in the "eye of the storm" explains why a patient may be in significant pain even when their X-rays and range-of-motion tests seem "normal."
Conclusion: A New Way to Look at the Mirror
Understanding these biomechanical quirks—from the paradoxical tilting of the Atlas to the "normal" fissures in our discs—fundamentally changes how we view neck health. We are moving away from seeing the neck as a simple stack of bones and toward seeing it as a complex, shifting gear system where "normal" is a moving target.
As we advance our understanding of clinical biomechanics, perhaps we should shift our focus. Instead of worrying about "how far" we can turn our heads, should we be looking more closely at "how well" the vertebrae are dancing together? Maintaining the quality of that movement—the stability of that "eye of the storm"—may be the true secret to a healthy, pain-free neck.